Heel bone fracture
Fractures of the heel bone, i.e., the largest bone of the foot are relatively common and account for about 2% of all bone fractures. They occur when falling from a great height, so the classic falling from a ladder or tree. Car accidents are also a common cause.
Diagnosis involves of course an X-ray, but it is especially important to do a CT, where all bone fragments and angle changes can be very well assessed.
Treatment
Only very undisplaced fractures can be treated with a plaster cast. All others must be operated on. The optimal time of surgery is 8-12 days after the accident, when the swelling has decreased. The so-called tibial joint angle or Böhler angle should be reconstructed as anatomically as possible. Only if and when the joint surfaces to the ankle bone (talus) and the cuboid bone, i.e. the lower and anterior ankle are recovered, can the result be considered positive.
In the case of not too severe fractures, using small stitches and a screw, reconstruction with almost intact skin (percutaneously) can be achieved. Fractures, which are composed of many fragments, or where there has been a break-in of the articular surfaces an open operation should be carried out, because the bone defect must be filled with either tissue bank bone or iliac bone. Here we use low profile plates, which with good stability protract very little and can usually be left.
Post treatment
Cast immobilization is usually 6 to 8 weeks. Afterwards, a special shoe is often necessary. In exceptional cases immobilization lasts for 12 weeks, for example in the case of extensive defects that needed to be filled. After the plaster cast, intensive physiotherapy is necessary.
Results
Calcaneal fractures are serious injuries and residual problems often remain for a certain time or long term. The better the reconstruction, the better the result. Good results occur in about 70% of cases, although often a restricted movement of the lower ankle joint remains.
Ability to work and do sports
Office workers can work in about 2-3 weeks. Physical labour and strenuous sport must be avoided for about 3 to 6 months depending on the severity of the injury as well as reconstruction.
Complications
In the case of open fractures, the risk of infection increases to about 7%, if it is closed around 3%. In addition to antibiotics, further operations to remove dead tissue are usually essential. Rarely does any part of the heel bone have to be removed. The risk that the fragments will not heal well without infection, is low. Wound healing impairment of soft tissue is relatively common, it being from about 5 to 10%.
Comminuted fracture of the calcaneus and its care



Left: only one fracture line is visible on the X-ray.
Middle & right: only on the CT is the true extent of the comminuted fracture visible (arrows).
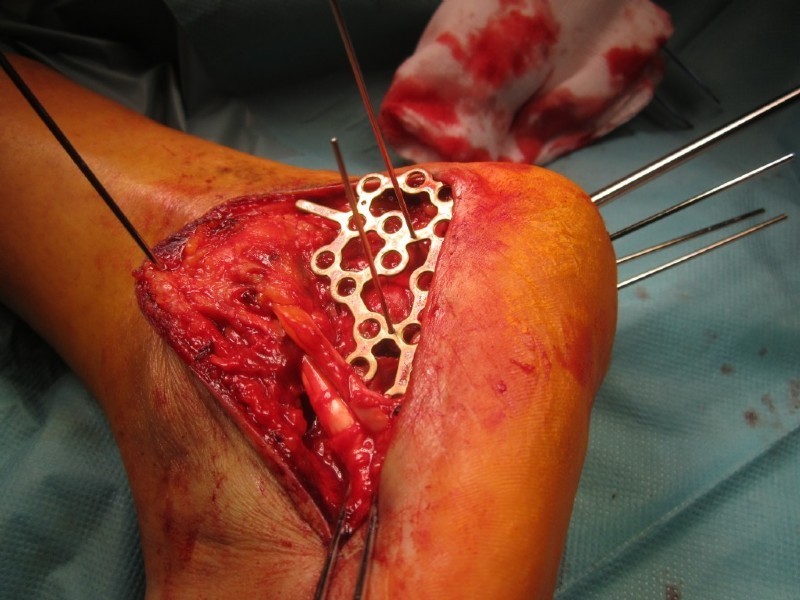
The open restoration of the calcaneal form (repositioning) is done with wires and rods.
The control of the result is attained by means of image converter. The stabilization is performed with a low profile heel bone plate. Nevertheless, immobilization in a lower leg cast is necessary for at least 6 weeks.


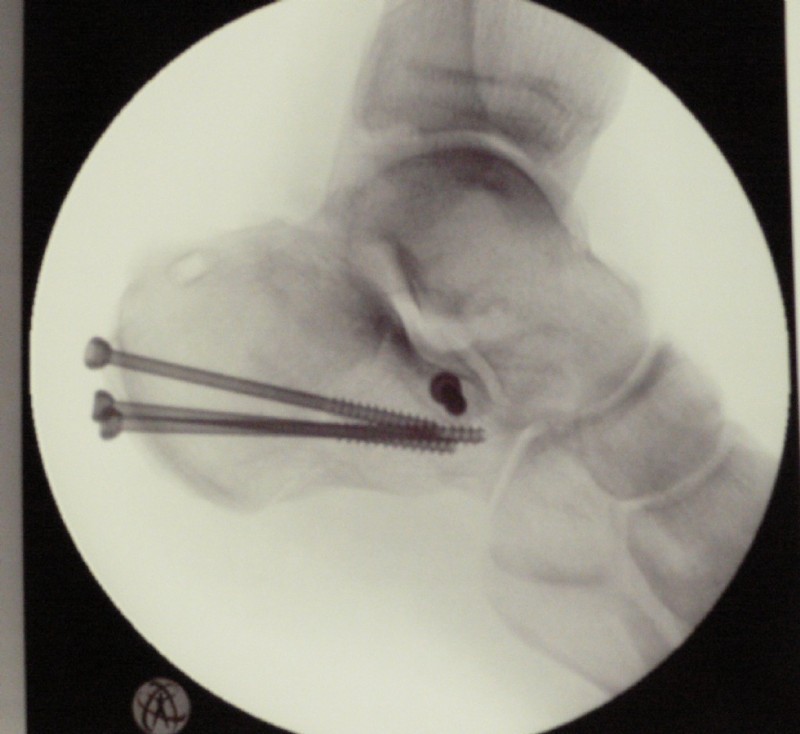
This calcaneal fracture was percutaneously repositioned, i.e. using small incisions under fluoroscopic view (restored) and stabilized with 4 screws.
Although the operation is much gentler, precise repositioning is not as feasible, as in open surgery, therefore making open surgery far more popular as the results are better.