Hammer Toes
Deformations of the small toes
Hammer toes are together with the bunion the most common deformities of the foot. For a long time now they have been treated surgically, as they sometimes cause excruciating pain in the shoe.
The most common operation in most hospitals - but not in ours - is the nearly 100 years old method described by Hohmann (1922), i.e. The removal of the joint forming bone part of the proximal phalange.
This operation is often performed independent of the type and condition of the toe, very often with fatal results.
The following disadvantages occur frequently:
- Very often, the gap closes due to connective tissue, causing a loose toe
- Not possible to bear full weight while walking
- Often disordered bone formations arise with renewed pressure points
- Often hammertoes re/emerge
- Lack of counter pressure by the second toes often causes deviation of the big toe - hallux valgus
It is important to distinguish between flexible and rigid or semi-rigid toes. Furthermore, it is of great importance for later results to examine if the toe is dislocated in the metacarpophalangeal joint, partly or entirely, and how long the toe is compared to the other toes, especially compared to the big toe, if there are tendon tensions and how the nature of the neighboring joints is.
Below we provide an overview of the surgical techniques we use, and also the undesirable results gained with surgery - done not in our units - when the rules of hammer toe surgery are disregarded.
Our current technique for the correction of hammer toes: minimally invasive bone cuts and tendon lenghtenings preserving all joints
We operate on hammertoes currently with 2 stab incisions of 2 to 3 mm length. This gives us excellent results, rapid recovery and no scars.
Example I:
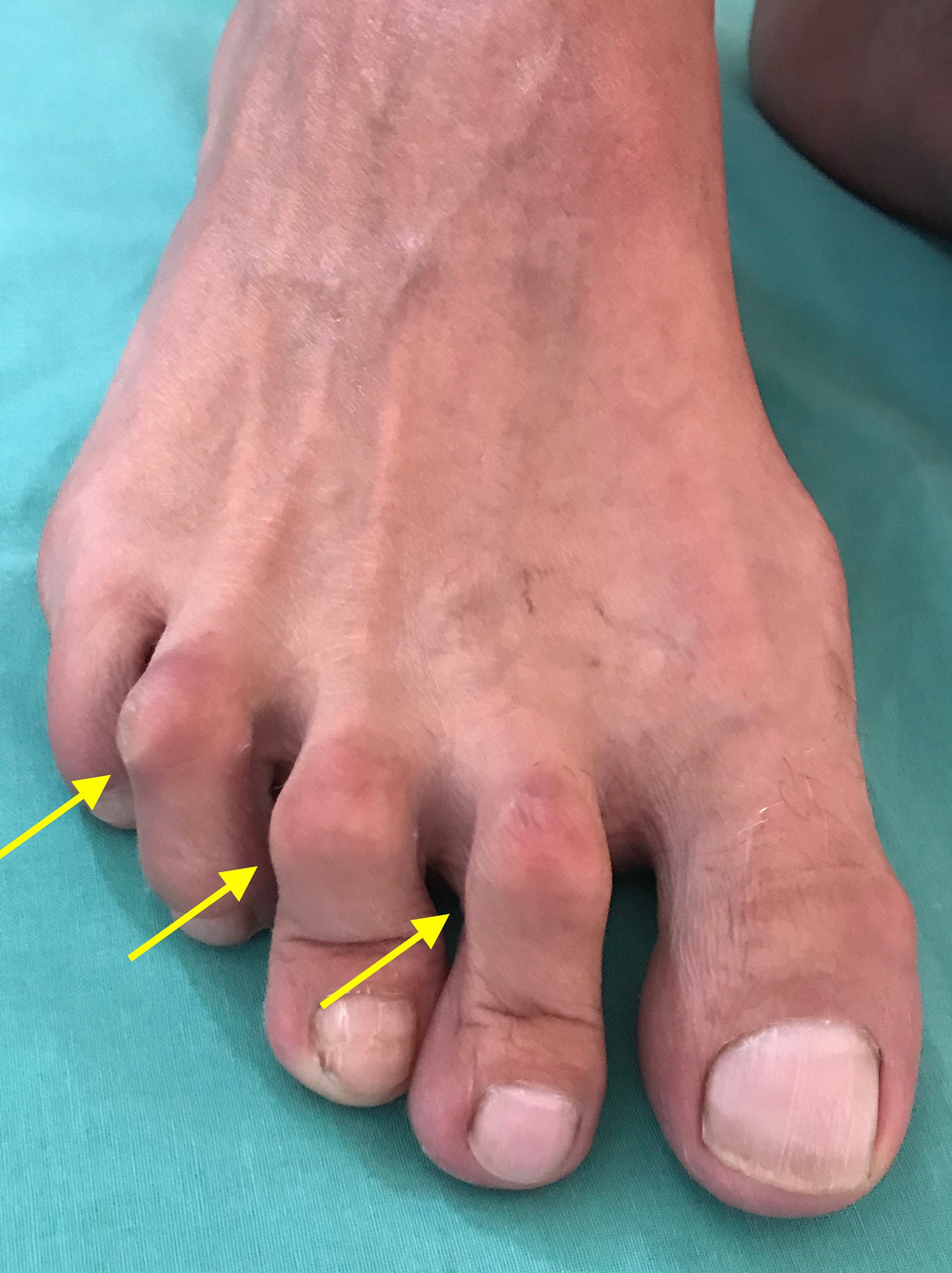
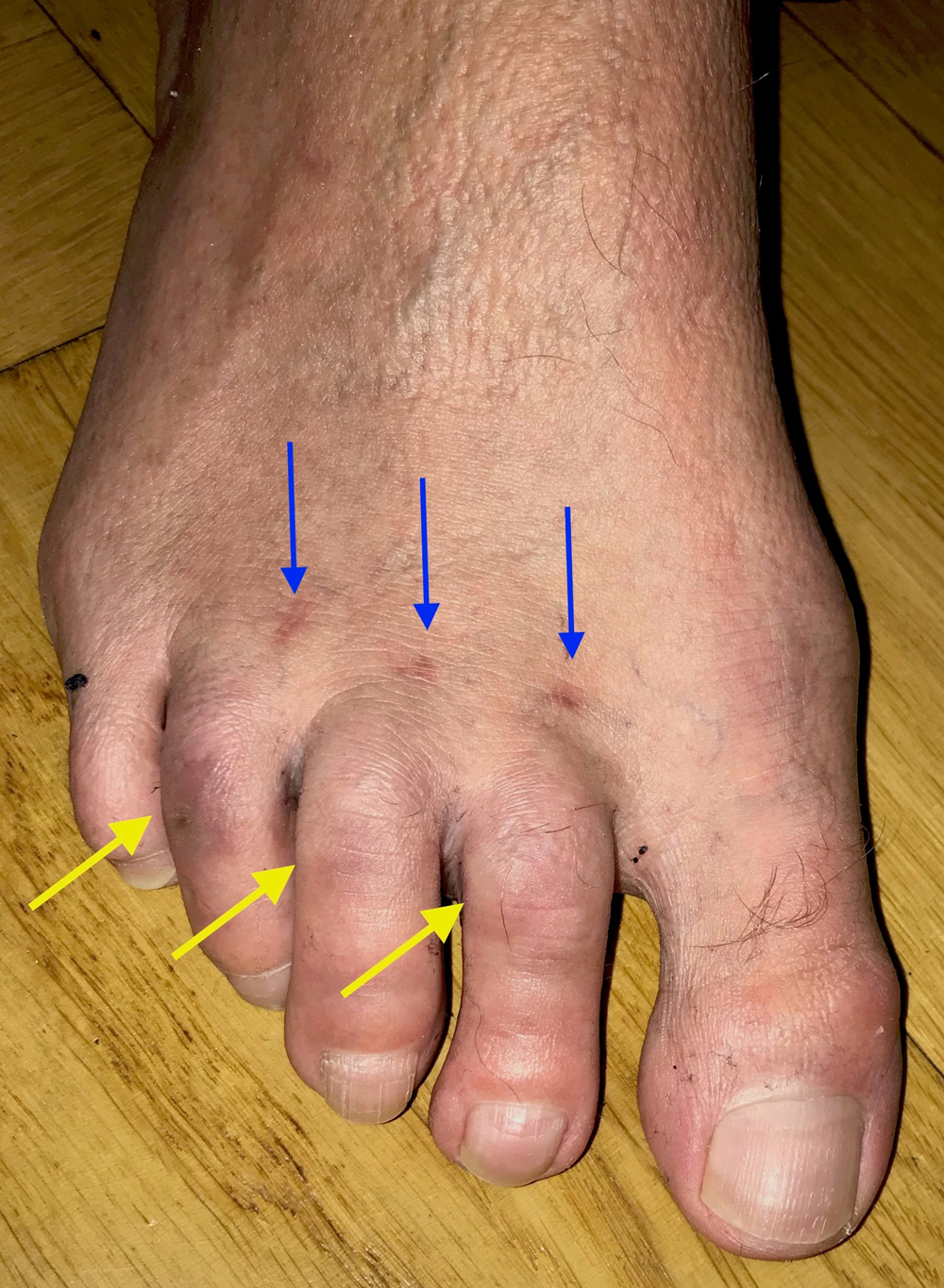
Patient W (male, 51 years), BEFORE: Severe pain in the ball of the foot (metatarsalgia) and pain and shoe problems on the side of massive hammer toes 2, 3 and 4 (yellow arrows).
AFTER: Result 6 months after the operation. All pain has disappeared. No bunion pain, no toe problems (yellow arrows). The hammer toes are straight and the calluses are gone. The tiny scars are now almost completely invisible (blue arrows).
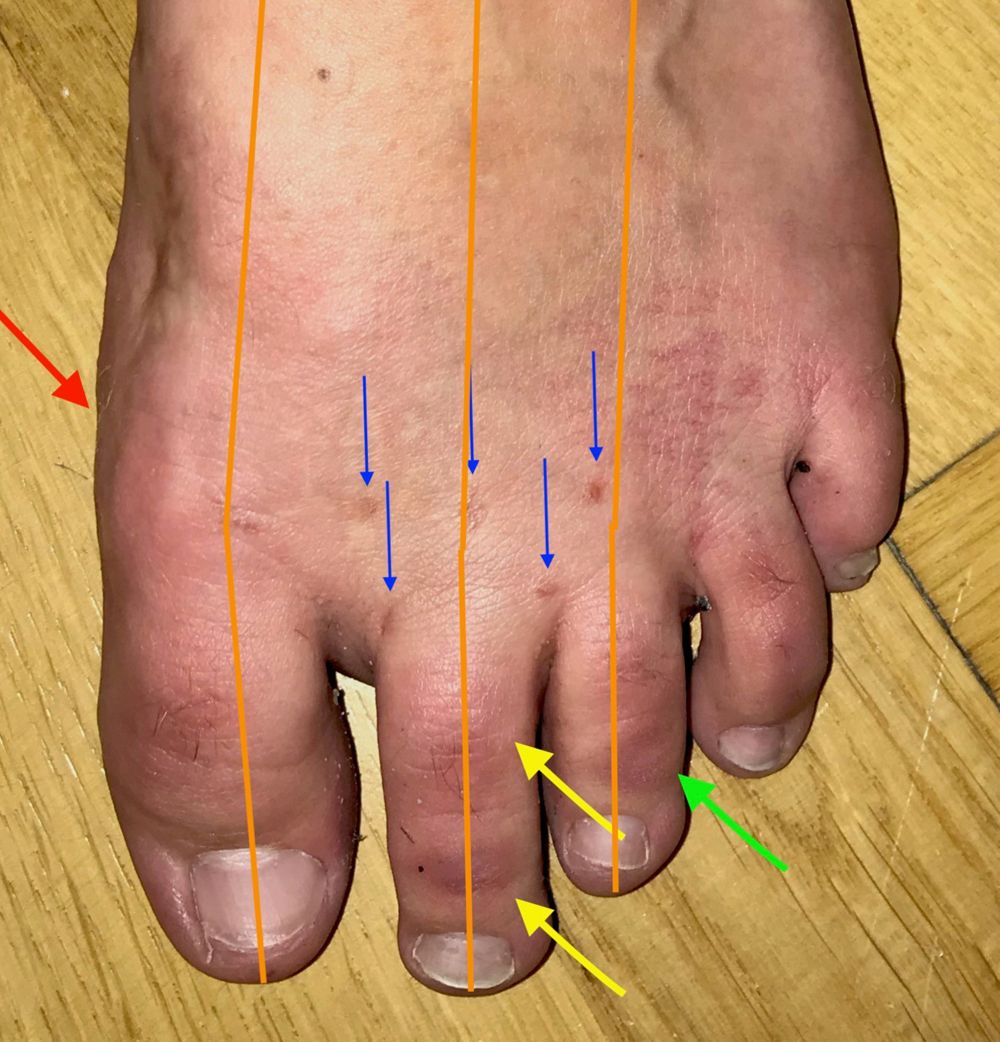
Example II:
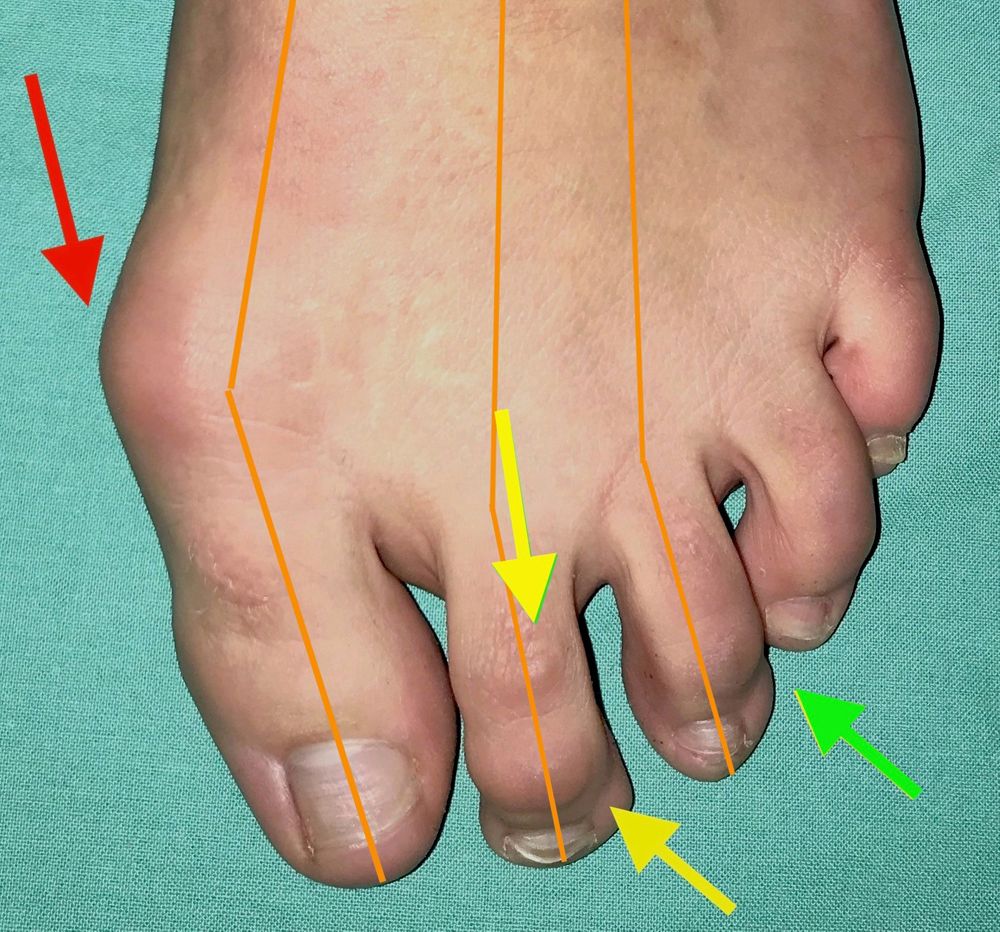
Patient XY (female, 26 years), BEFORE: The patient was operated elsewhere 2 years ago because of hallux valgus and came to me because she was very dissatisfied with the result. The hallux had come again (red arrow) and caused pain. In addition, hammer toes developed quickly (yellow arrows on the 2nd toe concerning both joints and on the 3rd toe concerning the end joint - green arrow). This happens quite often when the big toe loses most of its function due to its malposition. The axes of the toes 1, 2 and 3 deviate outwards (orange lines).
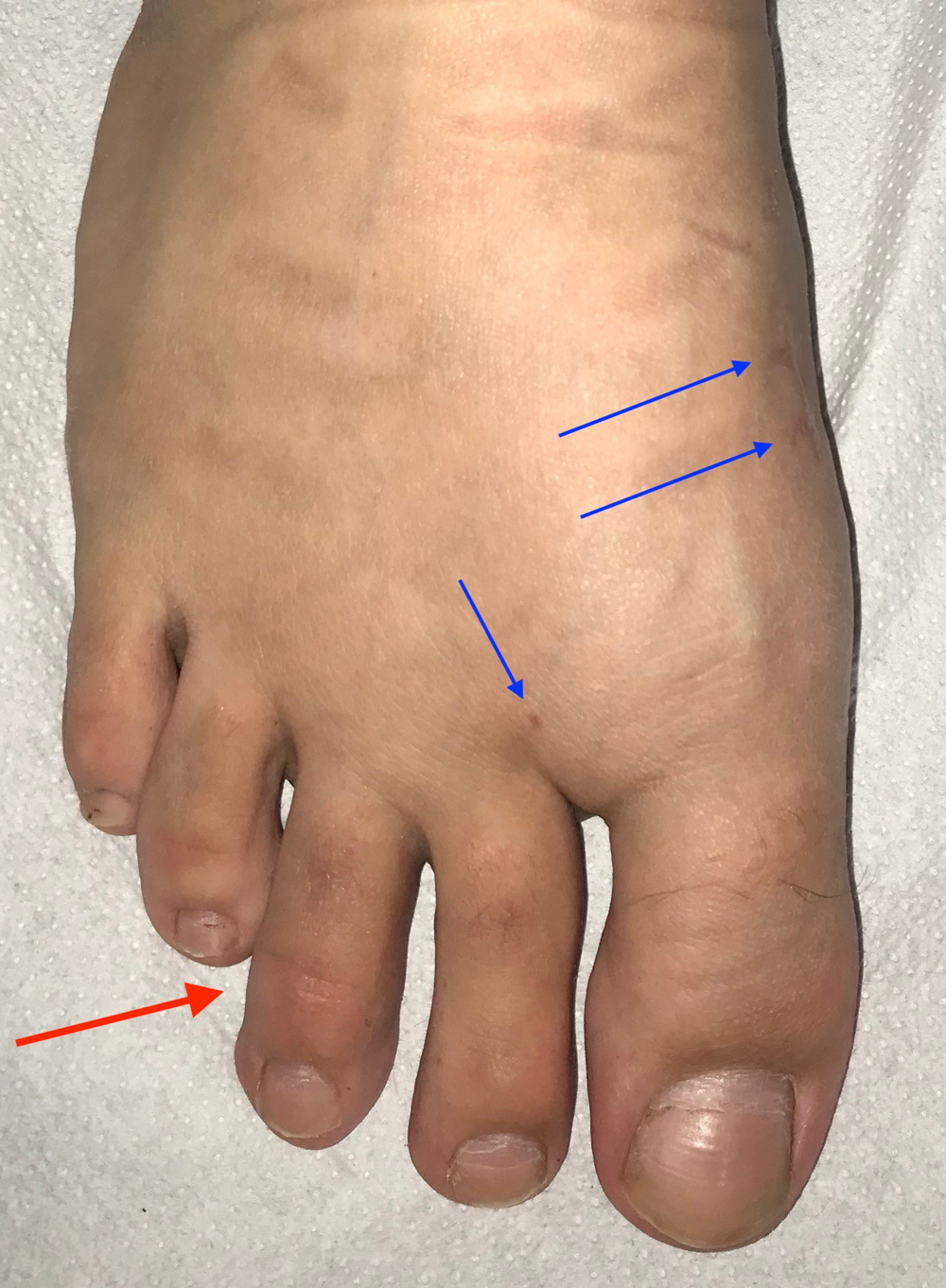
AFTER: 2 months after the correction at our clinic: The hallux is straightened and the bunion removed (red arrow). Toes 2 and 3 were also straightened in all joints (yellow and green arrows). All joints were preserved. Implants were only inserted during the hallux operation, toes 2 and 3 remained without implants. Please also note the axes of the toes 1, 2 and 3 (orange lines): These toes now no longer deviate outwards. The result will now be permanent, as no pathological lateral forces can occur anymore.
Example III:
Patient ZF (female, 68 years), BEFORE: A severely deformed foot. The big toe is strongly deviated (very pronounced hallux valgus) and also displaces the 2nd and 3rd toe. These cross over the 4th toe and form hammer toes. There is pain as well as problems finding shoes.
AFTER: Patient ZF (68 years) 8 weeks after the operation: All toes are in their ideal position and have been straightened. They now reach the ground well and can take part in the rolling process. The scar of the hallux operation is 15 mm and is hardly visible (not shown here). The scars on the back of the foot are also hardly visible (blue arrows). The swelling of the foot is already very low 8 weeks after the operation and this despite the very extensive procedure due to the massive malpositioning. The patient has been pain-free for a long time and is able to walk very well.


Example IV:
Patient U (female, 24 years), BEFORE: Slight but disturbing hallux valgus and a very disturbing hammer toe at the 3rd toe, a so-called distal hammer toe affecting the end joint (red arrow).
AFTER: Patient U (24 years) 6 weeks after surgery. The hallux was straightened and the 3rd toe was also straightened (red arrow). All scars are tiny (blue arrows). With the corrected 3rd toe, no scar at all is visible, it is on the underside. No pain, hardly any swelling and since the operation she can walk well.

Here we show examples of our older open techniques, which we use now only in exceptions.
1. Flexible (soft) hammer toes
In this deformity, the toe can be stretched manually, i.e. By the hand. Here it is sufficient to transfer the long flexor tendon to the toe phalanx. All joints are maintained. The toe does not lose its length, but it regains its function.
The technique was simplified by me and made secure by our interference screw, as it holds the offset tendon and you no longer have to rely on seams, which often used to lead to treatment failure.

Flexible, but annoying hammer toe (second toe).
Right: Ideal correction, the second toes can completely bear weight when walking, the corn is gone. In the X-ray you can see the screw which fastens the displaced tendon.
The second toe is completely off the ground and cannot be used while walking. In the shoe it also nudges at the top and causes pain.
After the correction of hallux valgus (big toe deformity) with the smallest cut and mini plate, space was created for the second toe and a tendon transfer using the new technology helped straighten the toe. A completely normal and healthy foot was the result.
2. Rigid (fixed) Hammer toes
Here you can not correct the deformity by hand, the toe rigidly remains in its flexed position.
To improve the to date often horrible results (especially my own - as of course I previously also used the usual clip-off technique), I developed a new method between 2003 and 2005 to stabilize the hammer and claw toes.
Since the toe in its deformity at the basal joint is stiff anyway, our operation purpose is to stiffen the joint in the straight position. A correction, in which the joint straightens and can be moved again, is no longer possible in case of rigid hammertoes.
This is not a disadvantage, however, as it only offers advantages:
- Definite solution, a hammer toe can not re-appear
- Predictable and reproducible results
- No protruding drill wires
- Full weight-bearing during walking and running is given
- No toe shortening
- Metal removal is not necessary
Therefore we use precise cutting guides that allow only the cartilage of the joint surface to be accurately removed. A massive reduction of the toe, as was customary upto now, is avoided!
New titanium micro-screws keep the correction intact until complete healing, which thanks to this technique is achieved in 2 to 4 weeks. Thereafter, a worsening of the situation is no longer possible, because the bone ends are solidly connected in the corrected position.
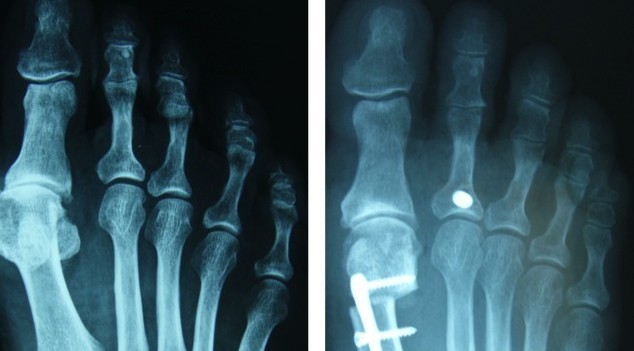
Example I


Left: bunion and rigid hammertoes / Right: After corrective surgery


Left: X-ray before surgery
Right: X-ray after correction of the hallux with the 30mm plate and correction of the rigid hammer toes II and III with micro screws
Example II
A foot operated upon elsewhere. The big toe deviates again (hallux valgus), is also twisted and the already operated hammer toe has re-emerged, but worse than before.




The foot and the X-ray images before and after the repair operation.
Example III
Solidly luxated (dislocated) and rigid hammertoe II, and a strongly developed hallux valgus make a comprehensive correction of the foot necessary.




Left: Before the surgery
Middle left: Already 3 weeks after surgery, the patient can wear normal comfort shoes and walk painlessly.
Middle right: The basal joint of the II toe is completely dislocated, the toe base (red arrow) is far away from the head (blue arrow). The head drills into the ground and causes severe pain when walking, which is also not controllable using insoles. The patient says it's "like walking on broken glass."
Right: After correction of hallux valgus, space was created for the second toe. Shortening of the metatarsal II and III (no Weil-surgery, but a joint-preserving one!). A tendon deviation so that the toe no longer rises and stiffening at the middle hinge. The toe can now support the standing and walking.
We DO NOT use the 3 minutes clip-off technique
Called the trochlear resection or Hohmann surgery or arthroplasty), where the connecting link joint is removed together with a centimeter or half of bone from the proximal phalanx of the toe:
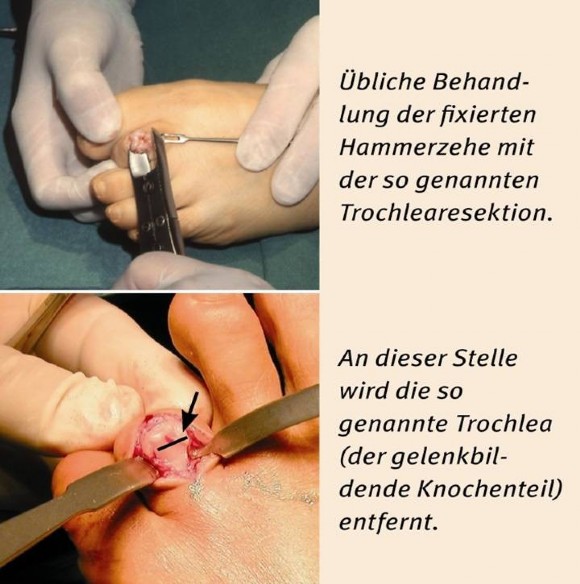
Common treatment of the fixated hammertoe with the so called trochlear resection.
At this point the so called trochlea (the joint-forming bone part) is removed.
Unfortunately, this surgical method is still used almost everywhere.
It is very fast and the result can be good initially. With time, however, it can often develop unsightly and painful toe deformities, some of which are shown here:

After hammer toe surgery:
At the second toe, a short time after surgery (clip off, medically called resection arthroplasty or trochlear resection) again a hammer toe emerged, an even shorter one. A new operation becomes much more difficult.
"The Wall of Shame" - undesired results after operations performed elsewhere
Some other examples from a large collection of images of hammer toes, treated using the shortening method (trochlear resection), I call this the "chamber of horrors":